smoking
food preservation
in food processing, the exposure of cured meat and fish products to smoke for the purposes of preserving them and increasing their palatability by adding flavour and imparting a rich brown colour. The drying action of the smoke tends to preserve the meat, though many of the chemicals present in wood smoke (e.g., formaldehyde and certain alcohols) are natural preservatives as well.
Smoking is one of the oldest of food preservation methods, probably having arisen shortly after the development of cooking with fire. The practice attained high levels of sophistication in several cultures, notably the smoking of fish in Scandinavia and northwestern North America and the production of smoked hams in Europe and the United States. Interest in smoking meats, which had declined during the mid-20th century owing to the popularity of chemical preservatives, was revived late in the century by the so-called natural or health food movement.
Whether done on a commercial or a home scale, the smoking technique involves hanging the meat or placing it on racks in a chamber designed to contain the smoke. Commercial smokehouses, usually several stories high, often use steampipes to supplement the heat of a natural sawdust fire. Hickory sawdust is the preferred fuel. Whatever the size of the smoking operation, it is imperative that a hardwood fire be used. The softwood of conifers such as spruce and pine contains pitch, which produces a film on the meat and imparts a bitter taste. Generally, smokehouse temperatures vary from 109° to 160° F (43° to 71° C), and smoking periods vary from as short as a few hours to as long as several days, depending on the type of meat and its moisture content. After smoking, the meat is chilled as rapidly as possible and cut and wrapped for the retail trade.
In the United States, pork and beef hams, bacon bellies, and sausages are the most common commercially smoked meats. However, amateurs using ordinary smoke ovens or adapting barbecue grills to the purpose have successfully used the smoking technique to flavour and preserve not only meat, fowl, and fish but also cheeses, nuts and seeds, hard-boiled eggs, and berries, as well as the variety meats including heart, tongue, and liver.
In order to shorten the production process, commercial meats are sometimes artificially “smoked” by dipping them in a solution of preservative chemicals or by painting them with such a solution. But because this procedure involves no natural drying action, it has practically no preservative effect.
tobacco
Introduction
the act of inhaling and exhaling the fumes of burning plant material. A variety of plant materials are smoked, including marijuana and hashish, but the act is most commonly associated with tobacco as smoked in a cigarette, cigar, or pipe. Tobacco contains nicotine, an alkaloid that is addictive and can have both stimulating and tranquilizing psychoactive effects. The smoking of tobacco, long practiced by American Indians, was introduced to Europe by Christopher Columbus and other explorers. Smoking soon spread to other areas and today is widely practiced around the world despite medical, social, and religious arguments against it.
Smoking and health
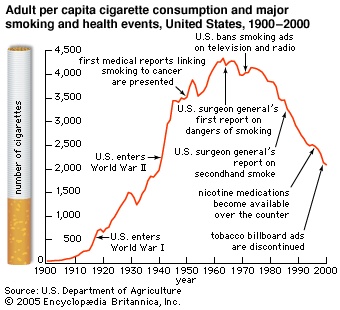
At the dawn of the 20th century, the most common tobacco products were cigars, pipe tobacco, and chewing tobacco. The mass production of cigarettes was in its infancy, although cigarette smoking was beginning to increase dramatically. According to the ninth edition of Encyclopædia Britannica (1888), tobacco products were suspected of producing some adverse health effects, yet tobacco was also considered to have medicinal properties. Many scholars and health professionals of the day advocated tobacco's use for such effects as improved concentration and performance, relief of boredom, and enhanced mood.
 By the dawn of the 21st century, in stark contrast, tobacco had become recognized as being highly addictive and one of the world's most devastating causes of death and disease. Moreover, because of the rapid increase in smoking in developing nations in the late 20th century, the number of smoking-related deaths per year is projected to rise rapidly in the 21st century. For example, the World Health Organization (WHO) estimated that in the late 1990s there were approximately 4 million tobacco-caused deaths per year worldwide. This estimate was increased to approximately 5 million in 2003 and could reach 10 million per year by the 2020s. By the mid-21st century, a staggering 500 million of today's cigarette smokers will have died prematurely because of their smoking. Although tobacco use is declining in many countries of western Europe and North America and in Australia, it continues to increase rapidly in many countries in Asia, Africa, and South America.
By the dawn of the 21st century, in stark contrast, tobacco had become recognized as being highly addictive and one of the world's most devastating causes of death and disease. Moreover, because of the rapid increase in smoking in developing nations in the late 20th century, the number of smoking-related deaths per year is projected to rise rapidly in the 21st century. For example, the World Health Organization (WHO) estimated that in the late 1990s there were approximately 4 million tobacco-caused deaths per year worldwide. This estimate was increased to approximately 5 million in 2003 and could reach 10 million per year by the 2020s. By the mid-21st century, a staggering 500 million of today's cigarette smokers will have died prematurely because of their smoking. Although tobacco use is declining in many countries of western Europe and North America and in Australia, it continues to increase rapidly in many countries in Asia, Africa, and South America. Major health effects of tobacco product by typeThe primary cause of the escalation in the number of deaths and incidents of disease from tobacco is the large increase in cigarette smoking during the 20th century. During that time cigarette smoking grew to account for approximately 80 percent of the world's tobacco market. Nonetheless, as is shown in the table (Major health effects of tobacco product by type), all tobacco products are toxic and addictive. In some regions of the world, the use of smokeless tobacco products is a major health concern.
Tobacco products are manufactured with various additives (food additive) to preserve the tobacco's shelf life, alter its burning characteristics, control its moisture content, inhibit the hatching of insect eggs that may be present in the plant material, mask the irritative effects of nicotine, and provide any of a wide array of flavours and aromas. The smoke produced when tobacco and these additives are burned consists of more than 4,000 chemical compounds. Many of these compounds are highly toxic, and they have diverse effects on health.
Health effects of primary smoke constituentsThe primary constituents of tobacco smoke are nicotine, tar (the particulate residue from combustion), and gases such as carbon dioxide and carbon monoxide. The effects of nicotine, tar, and carbon monoxide on health are summarized in the table (Health effects of primary smoke constituents). Although nicotine can be poisonous at very high dosages, its toxic effect as a component of tobacco smoke is generally considered modest compared with that of many other toxins in the smoke. The main health effect of nicotine is its addictiveness. Carbon monoxide has profound, immediate health effects. It passes easily from the lungs (lung) into the bloodstream, where it binds to hemoglobin, the molecule in red blood cells (erythrocyte) that is responsible for the transfer of oxygen in the body. Carbon monoxide displaces oxygen on the hemoglobin molecule and is removed only slowly. Therefore, smokers frequently accumulate high levels of carbon monoxide, which starves the body of oxygen and puts an enormous strain on the entire cardiovascular system (human cardiovascular system).
 The harmful effects of smoking are not limited to the smoker. The toxic components of tobacco smoke are found not only in the smoke that the smoker inhales but also in environmental tobacco smoke, or secondhand smoke—that is, the smoke exhaled by the smoker (mainstream smoke) and the smoke that rises directly from the smoldering tobacco (sidestream smoke). Nonsmokers who are routinely exposed to environmental tobacco smoke are at increased risk for some of the same diseases that afflict smokers, including lung cancer and cardiovascular disease. Clean-air laws that prohibit cigarette smoking are becoming widespread. In the 1980s and 1990s, such laws typically required that nonsmoking areas be established in restaurants and workplaces. However, the finding that toxins in environmental smoke could easily diffuse across large spaces led to much stronger bans. Since 2000 many cities, states, and regions worldwide, including New York City in 2003, Scotland in 2006, Nairobi in 2007, and Chicago in 2008, have implemented complete smoking bans in restaurants, taverns, and enclosed workplaces. In addition, entire countries have implemented smoking bans in workplaces or restaurants or, in some cases, in all public areas, including Ireland, Norway, and New Zealand in 2004 and France and India in 2008. In 2005 Bhutan became the first country to ban both smoking in public places and the sale of tobacco products.
The harmful effects of smoking are not limited to the smoker. The toxic components of tobacco smoke are found not only in the smoke that the smoker inhales but also in environmental tobacco smoke, or secondhand smoke—that is, the smoke exhaled by the smoker (mainstream smoke) and the smoke that rises directly from the smoldering tobacco (sidestream smoke). Nonsmokers who are routinely exposed to environmental tobacco smoke are at increased risk for some of the same diseases that afflict smokers, including lung cancer and cardiovascular disease. Clean-air laws that prohibit cigarette smoking are becoming widespread. In the 1980s and 1990s, such laws typically required that nonsmoking areas be established in restaurants and workplaces. However, the finding that toxins in environmental smoke could easily diffuse across large spaces led to much stronger bans. Since 2000 many cities, states, and regions worldwide, including New York City in 2003, Scotland in 2006, Nairobi in 2007, and Chicago in 2008, have implemented complete smoking bans in restaurants, taverns, and enclosed workplaces. In addition, entire countries have implemented smoking bans in workplaces or restaurants or, in some cases, in all public areas, including Ireland, Norway, and New Zealand in 2004 and France and India in 2008. In 2005 Bhutan became the first country to ban both smoking in public places and the sale of tobacco products.Health consequences of smoking
Addiction
A major health effect common to all forms of tobacco use is addiction, or, more technically, dependence. Addiction is not lethal in its own right, but it contributes to tobacco-caused death and disease, since it spurs smokers to continue their habit, which repeatedly exposes them to the toxins in tobacco smoke. Although there are many historical accounts of the apparent ability of tobacco use to escalate into an addiction for some smokers, it was not until the 1980s that leading health organizations such as the Office of the Surgeon General in the United States, the Royal Society of Canada, and WHO formally concluded that cigarettes are highly addictive on the basis of their ability to deliver large doses of nicotine into the lungs, from which blood quickly carries it to the brain.
Nicotine produces the entire range of physical and behavioral effects characteristic of addiction. These effects include activation of brain reward systems that create behavioral effects and physiological cravings that lead to chronic use, tolerance and physical dependence, and withdrawal upon discontinuation. Addiction to tobacco also involves a variety of constituents in tobacco smoke that, for many people, have pleasurable sensory characteristics and enhance nicotine's effects. Such constituents as ammonia, menthol, levulinic acid, and even chocolate improve a cigarette's flavour and aroma. Cigarettes are addicting, more so than nicotine medications, such as nicotine patches and gum, whose sensory and other effects are weaker and less desirable. (See below the section Smoking cessation (smoking).)
Deep inhalation of nicotine-laden smoke results in rapid absorption of nicotine in the lungs—the nicotine diffuses into the bloodstream as rapidly as the inhaled oxygen. From the lungs the nicotine reaches the brain in less than 10 seconds. Nerve cells, or neurons (neuron), in the brain and peripheral nervous system have receptor proteins (receptor) on their surfaces to which nicotine binds, much in the way that a key fits into a lock. When a molecule of nicotine binds to a nicotine receptor, it causes the neuron to transmit a nerve impulse to various target organs and tissues. This process stimulates the release of neurotransmitters (neurotransmitter), or chemical messengers, which produce the physiological and psychological effects of nicotine. For example, nicotine stimulates the adrenal glands (adrenal gland) and prompts the release of epinephrine and norepinephrine, which are responsible for raising heart rate and blood pressure and heightening alertness and concentration. Nicotine also stimulates the release of the neurotransmitter dopamine in the brain. Dopamine is thought to be critical to nicotine's reinforcing and pleasurable mood-altering effects.
Most smokers report that their initial experiences with smoking were far from pleasurable. The nicotine in tobacco can have toxic effects in first-time users, who commonly experience dizziness, nausea, and even vomiting. With experience, smokers become adept at limiting their dose of nicotine to one that provides its desired effects. With continued use of tobacco, however, the body creates more and more nicotine receptors. As a result, the smoker experiences a phenomenon called tolerance—greater amounts of nicotine are needed in order to experience the same effect. Typically, when tolerance has developed and nicotine intake has increased, the body becomes physiologically dependent on nicotine, and any abrupt abstinence from smoking will trigger withdrawal symptoms. These symptoms include impaired ability to concentrate, irritability, weight gain, depressed mood, anxiety, difficulty sleeping, and persistent cravings. The symptoms typically peak within a few days and subside within a month. However, the experience varies from person to person, and, for some, powerful cravings can persist for years.
Nicotine's ability to help tobacco users control their mood and appetite and sustain their attention when working undoubtedly contributes to the persistence of tobacco use. Some of these effects interact with physical dependence. For example, increased exposure to nicotine can increase physical dependence and thereby make the effects of withdrawal stronger. During withdrawal, resumption of smoking provides rapid relief of withdrawal effects. This reaction may lead the smoker to believe that smoking in itself enhances mood and performance, when in reality the effect is mainly that of reversing the withdrawal symptoms, which occur only because of the physical dependence on nicotine. This effect can be profound, at least from the smoker's perspective. For example, cigarette smokers generally weigh some 2 to 4 kg (4.4 to 8.8 pounds) less than nonsmokers, and weight gain frequently accompanies cessation of smoking. Resumption of smoking can help people lose the gained weight. Similarly, even a few hours of tobacco abstinence can leave some people unable to get their work done, study for an exam, or perform adequately in other ways. Over time the smoker may learn that even a single cigarette can provide an immediate restoration of performance.
All widely used tobacco products deliver addicting levels of nicotine. However, the patterns of use that can lead to addiction vary with different tobacco products and are affected by many factors. For example, simply raising the cost of and limiting access to tobacco products tend to reduce tobacco use (thereby reducing the risk of addiction) and can even prompt some addicted persons to quit smoking. cigar smoking and pipe smoking (pipe) tend to be taken up later in life than cigarette smoking, and cigar smokers and pipe smokers are less likely to inhale the smoke. As a consequence, the overall rate of addiction to cigars or pipes appears to be less than the addiction rate for cigarettes, although many cigar or pipe smokers undoubtedly become highly addicted. The highest risk of addiction to nicotine occurs when the drug is absorbed very rapidly, producing its noted pleasant psychoactive effects. Oral smokeless products, such as snuff and chewing tobacco, do not produce as rapid an effect on the brain as cigarette-smoke inhalation, but the convenience and ease of use of these products are appealing to many and contribute to their addicting effects.
cancer
It is estimated that approximately one-third of all cancer deaths worldwide are attributable to tobacco. Cigarette smoke contains more than 60 known carcinogens (carcinogen), including tobacco-specific nitrosamines and polycyclic aromatic hydrocarbons. Although certain of the body's enzymes metabolize carcinogens and cause them to be excreted, these enzymes sometimes function inadequately, allowing carcinogens to bind to cellular DNA and damage it. When cells with damaged DNA survive, replicate, and accumulate, cancers occur. Cancerous cells can metastasize—that is, travel to other sites in the body—causing the cancer to spread. Cancer risk is partly determined by the toxicity of tobacco products; however, the risk of disease is also strongly related to the amount and duration of toxin exposure. The longer and more frequently a person smokes, the more likely a tobacco-related cancer will develop. For this reason, addiction is a strong indirect contributor to other diseases in that it promotes high-level and persistent exposure to cancer-causing agents.
Since the majority of tobacco users are cigarette smokers who inhale smoke into the lungs, it is not surprising that active smoking and exposure to environmental tobacco smoke are believed to account for 90 percent of all cases of lung cancer. A marked increase in lung cancer has occurred in all countries of the world where smoking has increased. In the United States lung cancer is responsible for more cancer deaths than any other kind of cancer and kills more women each year than breast cancer. It is estimated that 85 percent of all cases of lung cancer could be prevented if all smoking of cigarettes stopped. However, exposure to carcinogens is not limited to the respiratory system. Smoking is a major cause of bladder cancer, pancreatic cancer, laryngeal cancer, oral cancer, and esophageal cancer. When a regular tobacco user successfully quits, the risk of cancer decreases, though not to the level of someone who has never smoked. Smokeless tobacco users, meanwhile, repeatedly expose the oral mucosa to toxins and have a substantially increased risk of getting head and neck cancers, though the risk depends in part on the period of consumption and the nature of the product. For example, Swedish smokeless tobacco (“snus”) is made to contain substantially lower levels of carcinogens than American smokeless tobacco, and the risk of tobacco-caused cancer in its users appears to be correspondingly lower. There are large geographic differences in the prevalence of oral tobacco use, with higher consumption in Sweden, India, Southeast Asia, and parts of the United States.
Lung disease
It is not surprising that smokers suffer from many respiratory diseases other than lung cancer. One such disease is chronic obstructive pulmonary disease, or COPD, which is one of the major causes of debilitation and eventual death in cigarette smokers. More than 80 percent of those diagnosed with COPD are smokers, and most of these people die prematurely, with a greater number of women dying from COPD than men. COPD is a general term that refers to respiratory diseases in which airflow is obstructed. Women's airways appear to be more sensitive to the effect of cigarette smoke. Women with COPD often experience greater breathlessness and a disproportionately greater thickening of airway walls relative to men with COPD. Most commonly, COPD refers to chronic bronchitis (chronic cough and phlegm production) and emphysema (permanent enlargement of air spaces accompanied by deterioration of lung walls), although specific diagnostic criteria sometimes differ. Active smoking and exposure to environmental tobacco smoke are also responsible for increases in other respiratory ailments, such as pneumonia, the common cold, and influenza. Smokers who contract these ailments take longer than nonsmokers to recover from them. Children are especially susceptible to the effects of environmental tobacco smoke. When raised in a household in which they are regularly exposed to environmental tobacco smoke, children are more likely to suffer from asthma and chronic cough, and they may suffer from reduced lung growth and function.
Heart disease
Smoking has long been recognized as a major risk factor in cardiovascular disease, the risk being greater the more one smokes. As previously discussed, the carbon monoxide present in cigarette smoke binds to hemoglobin in the blood, making fewer molecules available for oxygen transport. In addition, coronary blood flow is reduced, forcing the heart to work harder to deliver oxygen to the body. Such strain places smokers at significantly greater risk for myocardial infarction, or heart attack, and stroke. There are, however, regional differences in the incidence of smoking-related cardiovascular disease. In China, for example, where smoking rates have increased steadily since the 1970s and about 63 percent of adult males smoke (as opposed to 4 percent of adult females), cardiovascular disease makes up a much smaller percentage of smoking-related deaths than in the United States and Europe, where it accounts for approximately 30 to 40 percent of all tobacco-caused deaths. After quitting, a smoker's risk for cardiovascular disease falls faster than the risk for lung cancer, with reductions in risk evident within one year of cessation.
Effects on pregnancy
Women who smoke are more likely to experience infertility and miscarriage (spontaneous abortion). When a pregnant woman smokes, some toxins from the smoke can be passed to the fetus. These toxins can later affect an infant's lung development and lung function. Babies of women who smoke are more likely to be born prematurely, to have a low birth weight, and to have slower initial growth. Smoking cessation within the first trimester lowers these health risks to a level comparable to those of people who have never smoked. Infants in households where there is a smoker are more likely to die from sudden infant death syndrome (SIDS).
Smoking cessation
The starting point for “kicking the habit” is awareness of the harm smoking can cause. For example, after the U.S. surgeon general's report in 1964 brought to public awareness a link between smoking and cancer, smoking rates in the United States dropped precipitously. By 2000 the smoking rate was about one-half that of 1960. Furthermore, strong antismoking warnings and health-related messages generally increase smokers' motivation to quit, as was shown in Canada when it adopted strong graphic warnings on cigarette packaging. Such warnings are now promoted by WHO as an important educational tool to motivate smoking cessation and to help prevent persons from starting to smoke.
Unfortunately, the vast majority of people who try to stop smoking resume within a few weeks of quitting because of the addictive grip of nicotine. Persons who smoke any cigarettes at all usually smoke enough to develop an addiction to nicotine. In general, the more cigarettes a person smokes per day, the greater is the addiction and the more difficult it is to quit. In addition to nicotine dependency, other factors that impede quitting are easy access to cigarettes and the withdrawal symptoms that accompany any discontinuance of nicotine intake. These symptoms include cravings, depression, anxiety, irritability, difficulty concentrating, and insomnia.
Dependence and withdrawal can be managed better by some people than others, and people often learn how to deal with these problems after repeated attempts. Medical intervention, including behavioral guidance, can be critical for recovery from tobacco addiction; scientifically based treatment strategies can have more than double the success rate of quitting “cold turkey” without assistance. Because the health benefits of quitting are so profound, leading health authorities consider treatment for tobacco dependence to be among the most important and cost-effective types of medical intervention. WHO and the governments of many nations are working aggressively to make scientifically proven treatments available to all tobacco users so that they may find a path to better long-term health. Other organizations such as the World Bank are working to support the availability of treatment in developing countries so that their struggling economies are not crippled by tobacco-caused disease and its burdens on health care systems and worker productivity.
Behavioral intervention
Quitting successfully must generally start with a plan for managing behaviour associated with tobacco addiction. Common to virtually all therapeutic approaches is the selection of and planning for a quitting date and adherence to the plan. The plan should include strategies for avoiding or managing situations that might stimulate a craving for a cigarette and therefore trigger a relapse to smoking. For example, for a few weeks or months, some people will need to avoid certain places and activities that they associate with smoking. Others will find it useful to learn methods by which to cope with stress or occasional cravings, such as breathing deeply, chewing gum, or taking a brief walk. Major health organizations provide information on a variety of successful strategies that can be tailored to an individual's situation.
Social and emotional support is often critical in sustaining an individual's efforts to quit. Support can come from a structured smoking-cessation program with group, one-on-one, or telephone counseling. Counseling need not be time-consuming or expensive. Studies have shown that even very brief counseling—as little as three minutes total—can make a difference, although more extensive treatment is generally more effective. Support from family members, friends, and health professionals can also play an integral part in the process of quitting.
For many persons a nicotine medication that helps address the physical aspects of nicotine dependence and withdrawal can be as important and beneficial as medications used for the management of other disorders, such as high blood pressure, in which behavioral strategies are also important.
Nicotine replacement therapy
Nicotine replacement therapy delivers nicotine to the body in controlled, relatively small doses, typically by means of a transdermal patch, chewing gum, a nasal spray, an inhaler, or tablets. These products do not contain the tar, carbon monoxide, or other toxic ingredients that are largely responsible for the health hazards of smoking, and, because they deliver controlled doses of nicotine, they are much less addictive than cigarettes. All these products are comparably effective, and advice on making a selection can be obtained from health organizations, health professionals, and the providers of the therapy. In particular, pregnant women, adolescents, and people with heart disease should consult a health professional for advice on product selection and dosing.
In contrast to tobacco products, nicotine replacement medicines are safe when used as directed. They deliver lower doses of nicotine into the bloodstream and do so more slowly than tobacco products do. Nicotine is not a carcinogen or lung toxin, and the nicotine doses delivered by the medicines do not produce cardiovascular disease. Nicotine at higher doses than are typically prescribed can contribute to low fetal birth weight and other adverse effects during pregnancy; however, the benefit of increased success in smoking cessation for women of childbearing age who have already tried and failed to quit without medication is generally considered to outweigh this comparatively small risk. Nicotine medications carry a very low potential for establishing addiction, and there is little evidence of their abuse. Some people may find the use of medications vital for many months to preventing a relapse to tobacco use. Such individuals are generally encouraged to take the medications as long as required in order to be confident to avoid a relapse. In fact, the most common dosing error is taking too little or not using the medicine long enough. Taking too much can produce the same short-lived symptoms of dizziness, nausea, and headache that are associated with smoking too many cigarettes, but this generally is not a serious health concern.
Nicotine patch
Nicotine patches are available without a prescription in many countries. A new patch is applied to the skin every day and is left in place for a recommended amount of time (usually 16 to 24 hours) while it delivers a controlled amount of nicotine to the body through the skin. The patches are used over a period of six to eight weeks or longer. Patches with the highest dosage of nicotine (15 or 21 mg) are generally used for the first few weeks; patches with lower doses are used thereafter. The most common side effect of the nicotine patch is a mild itching, burning, or tingling at the site on which it is applied. The nicotine patch can produce sleep disturbances; if they persist, they can often be remedied by removing the patch at bedtime.
Nicotine gum and lozenges
Nicotine gum, usually available in 2- and 4-mg formulations, is available in many countries without a physician's prescription. The gum is chewed a few times and then placed between the cheek and gums to allow the nicotine to be absorbed through the mouth's mucous membrane. These actions are repeated for up to about 30 minutes. Achieving success with gum as a cessation aid depends largely on using it consistently. At least one piece of nicotine gum should be used every one to two hours over a period of one to three months. Additional pieces may be used in the event of a strong craving. Possible side effects include mouth soreness, headache, and jaw ache. Nicotine lozenges in 2- and 4-mg dosages are also available in many countries. The lozenges are similar to nicotine gum in use except that they are not chewed.
Nicotine nasal spray
Nicotine nasal spray was designed to deliver nicotine more rapidly than is possible with a patch or gum. It is available by prescription only because it appears to carry a somewhat higher cardiovascular risk and a potentially higher risk for abuse than other nicotine medications do. The 1 mg of nicotine commonly prescribed (a 0.5-mg dose squirted into each nostril) is rapidly absorbed by the nasal mucosa. Patients are encouraged to use at least 8 doses (16 sprays) per day for optimal efficacy but can use up to 40 doses per day, depending on their level of nicotine dependence. The most common side effects include nasal and throat irritation, watery eyes, and runny nose. The nicotine nasal spray is not recommended for persons with nasal or sinus conditions, certain allergies, or asthma.
Nicotine inhaler
The nicotine inhaler, which consists of a nicotine-filled cartridge and a mouthpiece, was developed in order to imitate the behavioral and sensory characteristics of smoking without mimicking the actual delivery of nicotine to the lungs. The user inhales nicotine vapour into the mouth. Most of the nicotine is absorbed through the oral mucosa. The amount of nicotine delivered depends on the number of inhalations and their intensity. Depending on their needs, patients are advised to use from 6 to 16 cartridges per day. Each cartridge contains 10 mg of nicotine, of which 4 mg is delivered and up to 2 mg absorbed by the user. Side effects usually involve local irritation of the throat, together with coughing or sneezing. In most countries the nicotine inhaler is available only by prescription.
Sublingual nicotine tablets
The sublingual nicotine tablet is approved for use in several European countries. Each tablet commonly contains 2 mg of nicotine and is placed under the tongue until it dissolves; the nicotine is absorbed through the oral mucosa. Common side effects include irritation in the throat or under the tongue. As with nicotine gum, patients are instructed to move the tablet around within the mouth in order to alleviate these symptoms. The tablet form of nicotine is available without a prescription in many countries, but it is not available in the United States.
Bupropion
The first nonnicotine medication to gain approval for smoking cessation was the prescription drug bupropion, which was placed on the market in the United States in 1997 under the name Zyban. (The drug is also marketed as an antidepressant under the name Wellbutrin.) Bupropion seems to reduce both withdrawal symptoms and the urge to smoke by affecting the neurotransmitters dopamine and norepinephrine. Bupropion is available in the form of a 150-mg pill taken once a day for three days, then twice a day for 7 to 12 weeks, often concurrently with a nicotine replacement medication. Bupropion is not recommended for anyone who has a seizure disorder, has ever been diagnosed with an eating disorder, or takes certain kinds of antidepressants. Of the few major side effects that have been reported, insomnia and dry mouth are the most common.
Other approaches to smoking cessation
The most common approach to smoking cessation is that of quitting “cold turkey,” which is the sudden discontinuation of smoking. This approach is rarely effective the first time it is tried, but through repeated efforts some people eventually succeed by this approach. Yet many people might have been able to quit years earlier by using a proven form of treatment. Hypnosis, acupuncture, herbal remedies, and other approaches are often advertised as ways to help quit smoking. These methods have not been proved to be any more effective than simply deciding to quit, although some individuals undoubtedly have been able to quit smoking by using them. For people with physical withdrawal symptoms, such as an impaired ability to function in the workplace (many people have difficulty concentrating on tasks), strong proven methods may be the best road to success. Nonetheless, new techniques and medicines are constantly being evaluated, so people interested in quitting should consider checking with WHO or the various national cancer organizations for information. Treatments that are under development or consideration include a vaccine to help people refrain from smoking once they have quit smoking, a medication to help prevent weight gain associated with nicotine withdrawal, and a medication to help persons reduce tobacco use when they find that they cannot abstain from it.
Smoking and public policy
 For centuries, a major factor in setting public policy regarding tobacco products was the economic importance of the tobacco industry. Therefore, despite occasional efforts to prohibit the production of tobacco products, the main impetus of tobacco regulation throughout the world was to ensure the continued viability of the tobacco trade and to collect taxes on its products. The specific regulatory framework varied from country to country, but the result was essentially the same everywhere: tobacco was exempt from the ordinary controls to which other products were subject. In the United States, for example, tobacco products, which fell under the jurisdiction of the Bureau of Alcohol, Tobacco and Firearms, were exempt from the most basic safety and health standards required of other consumer products.
For centuries, a major factor in setting public policy regarding tobacco products was the economic importance of the tobacco industry. Therefore, despite occasional efforts to prohibit the production of tobacco products, the main impetus of tobacco regulation throughout the world was to ensure the continued viability of the tobacco trade and to collect taxes on its products. The specific regulatory framework varied from country to country, but the result was essentially the same everywhere: tobacco was exempt from the ordinary controls to which other products were subject. In the United States, for example, tobacco products, which fell under the jurisdiction of the Bureau of Alcohol, Tobacco and Firearms, were exempt from the most basic safety and health standards required of other consumer products.This state of affairs began to change in the early 1960s, when the United Kingdom's Royal College of Physicians (in 1962) and the U.S. surgeon general (in 1964) concluded that cigarette smoking caused lung cancer and other diseases. These reports were based largely on the rapidly mounting evidence from laboratory studies of smoke toxins and from population studies of disease risk in cigarette smokers in the 1950s. The reports paved the way for scientifically based health considerations to emerge as significant factors in the creation of tobacco public policy. Initial efforts were often aimed at specific issues, such as how tar and nicotine in cigarettes should be measured and advertised, health warnings on cigarette packaging, and smoking-prevention programs for young people. These limited efforts were generally thwarted or weakened by tobacco interests. Nonetheless, smoking by adults began to subside in the 1970s and 1980s in many developed countries, particularly in the United States, Canada, Sweden, and Australia. At the same time, the prevalence of smoking was rapidly increasing in many less-developed countries, particularly in Asia and Africa. By the 1990s the toll in death and disease in these countries was mounting rapidly, and youth smoking began to shoot upward in some of the countries, including the United States and Canada, that had shown great strides in the reduction of smoking in the 1970s and 1980s.
In the 1990s several currents converged to foster major smoking-control policy initiatives around the world. The leading current was an extensive body of scientific research that proved the deadly and addictive effects of tobacco beyond the ability of even the tobacco industry to deny. This included evidence that environmental smoke was more than an annoyance—it was lethal for thousands of nonsmokers and a cause of respiratory disease in children. A second current was the sheer magnitude of the economic losses projected to be caused by tobacco use, as measured by the diversion of health care funds for the treatment of tobacco-related illnesses and by the loss of worker productivity. A third current was litigation brought against the tobacco industry by governments and individuals. These lawsuits brought to light millions of secret documents showing that the tobacco industry had long known its products were highly addictive and deadly. Finally, the growing recognition that environmental tobacco smoke was deadly even for nonsmokers led to efforts to restrain and contain smoking. These efforts further decreased smoking rates, making it possible for even stronger regulatory actions to be taken.
By the end of the 20th century, therefore, organized campaigns had led to the implementation of a wide spectrum of tobacco-related measures, including increases in the price of cigarettes and restrictions on their availability, restrictions in advertising, disclosure of information on the health consequences of tobacco use, protection of nonsmokers from environmental tobacco smoke, and regulation of manufacturing standards for tobacco companies. In the many countries that implemented such measures, per capita cigarette consumption was much reduced from earlier decades. However, in many developing countries and in the world as a whole, cigarette consumption continued to increase. In response to this increase, the World Health Organization (WHO) and other health organizations sought to step up coordinated international efforts to regulate tobacco products in the late 1990s. In 2003 WHO adopted a tobacco-control treaty designed to serve as an international framework for tobacco regulation. It imposed controls over tobacco-industry marketing, required health-warning labels on tobacco products, and sought to reduce the exposure of users and nonusers alike to tobacco toxins. The treaty was ratified at a rapid pace by many countries, and it entered into force in early 2005. Although some major countries, including the United States and China, had not ratified it by that time, more than one-third of the signatory countries had done so, including Canada, Japan, the United Kingdom, and many developing countries.
The goals and strategies of public policy on smoking
The goal of policy interventions on smoking is to reduce as rapidly as possible the incidence of death and disease related to smoking. Toward that end, policy measures employ a four-part strategy: (1) discourage individuals from starting to use tobacco, (2) encourage users to quit and provide support for their efforts, (3) reduce the adverse health consequences of tobacco by substantially reducing the toxins to which users are exposed through their use of tobacco products, and (4) expand clean-air nonsmoking policies to protect nonsmokers and to support prevention and cessation efforts.
No single action can accomplish these goals, but the coordination of a number of actions has proved effective in reducing tobacco use in a number of countries. These actions, encouraged by WHO, include:
● Reducing access to tobacco products by prohibiting sales to minors, raising prices, and making them more difficult to purchase.
● Promoting educational campaigns that provide detailed health information and ensuring that tobacco products include appropriate health warnings and information on how to get help in quitting.
● Restricting smoking in public areas and the workplace in order to protect nonsmokers. This action also has the effect of making it difficult to smoke and increases the pressure on smokers to quit.
● Regulating product manufacture to minimize the health risks to which tobacco users are exposed.
These goals and strategies may seem simple, but they are complex in practice because of opposition by the tobacco industry, merchants, and benefactors of tobacco sales. Furthermore, users of tobacco tend to find many reasons to keep using it and to oppose efforts to restrict it. Controlling access to tobacco products involves balancing efforts to prevent young people and nonusers from becoming tobacco users while continuing to make the products available to users. Efforts to inform consumers more thoroughly about the risks of use and the benefits of nonuse raise practical questions of how this information can be communicated most effectively to the consumer and what role, if any, the manufacturers should have in communicating such information.
Regulation
Regulation of the design and ingredients of tobacco products is perhaps the greatest challenge for tobacco-control advocates. In the United States the Food and Drug Administration in 1996 attempted to regulate tobacco and its marketing—without banning it—in such a way that would reduce smokers' risks of developing a nicotine addiction and increase their likelihood of quitting. Key elements of the regulation were increased restrictions on appeal-enhancing marketing and reduced access by young people to tobacco products. Although this regulatory effort was overturned by the U.S. Supreme Court in 2000, the court recognized that some form of substantial regulation was not prohibited by the Constitution.
The need to protect nonsmokers from the health risks of environmental tobacco smoke has led to stricter regulation of smoking in public places, such as airports and hotels, and even to citywide and countrywide bans on smoking in enclosed workplaces, including offices, restaurants, and taverns. Although the primary purpose of smoking restrictions is to prevent nonsmokers from being exposed to environmental tobacco smoke, a major public health benefit is that such restrictions put pressure on smokers to quit and, in general, act as a deterrent to smoking.
taxation
Price has likely been the single most effective policy intervention by those seeking to reduce tobacco-caused death and disease. Detailed studies have shown that in many countries price increases cause many smokers to quit and others to reduce their smoking. The smoking practices of young people have been shown to be particularly sensitive to price. For example, between 1982 and 1992 Canada raised the real price of tobacco products by 150 percent. This price increase coincided with a reduction in total cigarette consumption of roughly 40 percent and a reduction in teenage smoking of 60 percent. In some countries, including Australia and France, increases in cigarette prices have been found to be a potent force for preventing young people from taking up tobacco and for supporting smoking-cessation efforts among adults.
Litigation against the tobacco industry
Litigation and the threat of litigation played a major role in shaping the environment for tobacco products at the end of the 20th century. While litigation seeks to accomplish the same ends as legislation, it is often a more viable strategy in regions where legislators are reluctant to act against the interests of the tobacco industry and its frequent allies, such as convenience stores and the alcohol-selling portions of the hospitality industry, which rely heavily on tobacco sales for their total revenue.
Litigation covers a wide range of issues, including product liability, consumer protection, antitrust activity, racketeering, health care reimbursement, and tax evasion. These lawsuits have been brought forward by individuals, classes of individuals (class actions), governments, and others. The ability of plaintiffs to sue tobacco companies for health care reimbursement is based on various legal theories of recovery, including negligence, gross negligence, strict liability, fraud, misrepresentation, design defect, failure to adequately warn, and conspiracy. In a landmark 1998 case, the major cigarette companies in the United States entered into an agreement with the attorneys general of a number of states as a result of lawsuits aimed at recouping health care expenditures for treating sick smokers. This agreement required the disclosure of millions of corporate documents, the discontinuation of various forms of youth-focused advertising, and the annual payment in perpetuity of roughly $10 billion per year. Although the actual payment may vary and even decrease as cigarette consumption decreases, such a substantial amount has put pressure on tobacco companies to support legislative efforts they formerly opposed, since further litigation could bankrupt them.
A social and cultural history of smoking
In order to explain why enormous sections of the world's population continue to smoke, given the overwhelming medical evidence of its dangerous effects, one must understand the social history of the practice, the role of smoking in everyday cultural practices, and the meaning that people attach to it. Historian Jordan Goodman has argued that societies in which tobacco has been introduced have demonstrated a “culture of dependence,” be it in the ceremonial rituals of Native American culture, the fiscal policies of early modern states, the coffeehouses of 18th-century Europe, or the physical and psychological addictions associated with the cigarette. This dependence is one of the reasons individuals—and societies as a whole—are aware that smoking is harmful yet continue to smoke because of the individual and communal pleasures it brings. Smoking might represent folly and foolhardiness, but its intangible qualities still encourage millions to smoke. As the dramatist Oscar Wilde (Wilde, Oscar) wrote,
A cigarette is the perfect type of a perfect pleasure. It is exquisite and it leaves one unsatisfied. What more can one want?
Tobacco in New World culture
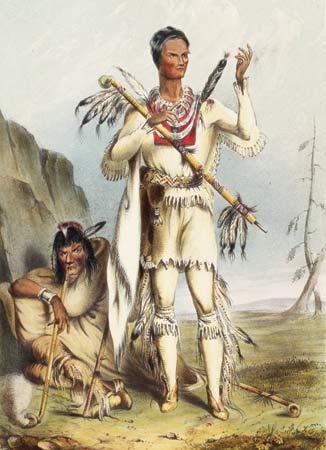 Although the origin of tobacco use in Native American culture (American Indian) is uncertain, tobacco clearly played a far more ceremonial and structured role than it would come to play in Europe and the modern world. Along with several other hallucinogens and narcotics, a strong, dark, high-nicotine and, consequently, mind-altering tobacco was crucial to the performance of shamanistic rituals (shamanism) and social ceremonies. Usually smoked but also chewed, drunk, taken as snuff, and even given as an enema, tobacco was seen by Native Americans (American Indian) as a means for providing communication with the supernatural world through the medium of the shaman, for either medicinal or spiritual purposes. Among other medical applications, tobacco was used as a cure for toothache by the Iroquois, as a cure for earache by the Indians of central Mexico, as a painkiller by the Cherokee, and as an antiseptic in Guatemala. Beyond such practical functions, tobacco was also often exchanged as a gift, helping to forge social connections and establish community hierarchies. In many groups tobacco was given as an offering to the gods, and in some groups, in particular among the Maya, tobacco was itself deified as a divine plant. Tobacco was also linked to the fertility both of the land and of women, and it was used in initiation ceremonies for boys entering manhood. Most famously, tobacco was used in the calumet ritual, when agreements and obligations would be made binding with the passing of the ritual pipe (the calumet, or Sacred Pipe). Tobacco was thus central to Native American culture, be it with the cigar in the South or the pipe in the North, and its properties were known from Canada to Argentina and from the Atlantic to the Pacific. So important was it that some native groups, such as the Blackfoot and the Crow, cultivated no other crop.
Although the origin of tobacco use in Native American culture (American Indian) is uncertain, tobacco clearly played a far more ceremonial and structured role than it would come to play in Europe and the modern world. Along with several other hallucinogens and narcotics, a strong, dark, high-nicotine and, consequently, mind-altering tobacco was crucial to the performance of shamanistic rituals (shamanism) and social ceremonies. Usually smoked but also chewed, drunk, taken as snuff, and even given as an enema, tobacco was seen by Native Americans (American Indian) as a means for providing communication with the supernatural world through the medium of the shaman, for either medicinal or spiritual purposes. Among other medical applications, tobacco was used as a cure for toothache by the Iroquois, as a cure for earache by the Indians of central Mexico, as a painkiller by the Cherokee, and as an antiseptic in Guatemala. Beyond such practical functions, tobacco was also often exchanged as a gift, helping to forge social connections and establish community hierarchies. In many groups tobacco was given as an offering to the gods, and in some groups, in particular among the Maya, tobacco was itself deified as a divine plant. Tobacco was also linked to the fertility both of the land and of women, and it was used in initiation ceremonies for boys entering manhood. Most famously, tobacco was used in the calumet ritual, when agreements and obligations would be made binding with the passing of the ritual pipe (the calumet, or Sacred Pipe). Tobacco was thus central to Native American culture, be it with the cigar in the South or the pipe in the North, and its properties were known from Canada to Argentina and from the Atlantic to the Pacific. So important was it that some native groups, such as the Blackfoot and the Crow, cultivated no other crop.Tobacco in Old World culture
 It is likely that sailors returning from the Americas to various ports in Europe in the late 15th and early 16th centuries took with them the practice of smoking. Northern Europeans adopted the practice of pipe smoking, which was prevalent along the north Atlantic seaboard, and Spaniards brought the practice of cigar smoking, which was prevalent in the regions around the Caribbean. Many Europeans believed tobacco was a panacea, a new herb that could be incorporated into Western medical traditions and celebrated as an almost universal curative. In the late 16th century, the Spanish doctor Nicolas Monardes claimed that tobacco alleviated hunger, acted as a relaxant and a painkiller, and was even a cure for cancer. However, this view was opposed by others, including King James I of England. James's Counterblaste to Tobacco, published in 1604, described smoking as “a custom loathsome to the eye, hateful to the nose, harmful to the brain, dangerous to the lungs, and in the black, stinking fume thereof, nearest resembling the horrible Stygian smoke of the pit that is bottomless.” Elsewhere, Popes Urban VIII and Innocent IX issued papal bulls excommunicating those who snuffed in church, the Ottoman sultan Murad IV made smoking a capital offense, and Russians were subject to having their noses cut off if caught smoking. Nevertheless, the acceptance of tobacco into Old World culture was assisted by the patronage it received from various aristocrats and rulers. For example, tobacco was introduced into the court of Catherine de Médicis in 1560 by Jean Nicot (from whom nicotine and tobacco's botanical name, Nicotiana tabacum, get their name) and into the court of Elizabeth I by Sir Walter Raleigh (Raleigh, Sir Walter), who himself had been introduced to smoking by Sir Francis Drake (Drake, Sir Francis).
It is likely that sailors returning from the Americas to various ports in Europe in the late 15th and early 16th centuries took with them the practice of smoking. Northern Europeans adopted the practice of pipe smoking, which was prevalent along the north Atlantic seaboard, and Spaniards brought the practice of cigar smoking, which was prevalent in the regions around the Caribbean. Many Europeans believed tobacco was a panacea, a new herb that could be incorporated into Western medical traditions and celebrated as an almost universal curative. In the late 16th century, the Spanish doctor Nicolas Monardes claimed that tobacco alleviated hunger, acted as a relaxant and a painkiller, and was even a cure for cancer. However, this view was opposed by others, including King James I of England. James's Counterblaste to Tobacco, published in 1604, described smoking as “a custom loathsome to the eye, hateful to the nose, harmful to the brain, dangerous to the lungs, and in the black, stinking fume thereof, nearest resembling the horrible Stygian smoke of the pit that is bottomless.” Elsewhere, Popes Urban VIII and Innocent IX issued papal bulls excommunicating those who snuffed in church, the Ottoman sultan Murad IV made smoking a capital offense, and Russians were subject to having their noses cut off if caught smoking. Nevertheless, the acceptance of tobacco into Old World culture was assisted by the patronage it received from various aristocrats and rulers. For example, tobacco was introduced into the court of Catherine de Médicis in 1560 by Jean Nicot (from whom nicotine and tobacco's botanical name, Nicotiana tabacum, get their name) and into the court of Elizabeth I by Sir Walter Raleigh (Raleigh, Sir Walter), who himself had been introduced to smoking by Sir Francis Drake (Drake, Sir Francis). After tobacco's introduction into Europe, the smoking and cultivation of it rapidly spread to other parts of the world. By the beginning of the 17th century, tobacco was being grown in India, China, Japan, Southeast Asia, the Middle East, and West Africa. With the availability of inexpensive clay pipes, tobacco became an item of mass consumption in England as early as 1670. Pipe manufacture spread throughout Europe. By the end of the 18th century, Dutch towns such as Gouda could support 350 pipe manufacturers, thanks to the smoking culture of coffeehouses and alehouses. snuff also proliferated, often rivaling smoking as the dominant form of tobacco consumption and producing such fascinating novelties as the perhaps apocryphal but frequently cited special pockets in the clothes of Frederick the Great (Frederick II) of Prussia, which were enlarged to cope with his considerable consumption. In southern Europe the great state-owned tobacco factories of Cádiz and Sevilla ensured the continued popularity of the cigar, though it was not until the Peninsular War (1808–14) that military officers began to popularize it in Britain. When pipes (pipe) were introduced into Asia, they were quickly adapted and made from materials as diverse as wood, bamboo, jade, ivory, metal, and porcelain. Arab communities took up the hookah, or water pipe, and smoking became a shared activity typically enjoyed with conversation and coffee. The hookah spread throughout Persia (present-day Iran) and into India, eventually reaching China, Southeast Asia, and many parts of Africa by the end of the 17th century. By the mid-19th century, smoking had become an established ritual throughout the world. It was celebrated in prose, in verse, in art, and on the stage, and its use came to be seen as a central component of manhood. Literary sources captured the paraphernalia of the smoking ritual—pipes, cleaners, holders, spills, spittoons, ashtrays, pouches, storage jars, and lighters, as well as smoking jackets, armchairs, hats, and slippers—all of which, ideally, had to be collected in “that chamber of liberty, that sanctuary of the persecuted, that temple of refuge… the smoking room” ( Ouida, Under Two Flags, 1867).
After tobacco's introduction into Europe, the smoking and cultivation of it rapidly spread to other parts of the world. By the beginning of the 17th century, tobacco was being grown in India, China, Japan, Southeast Asia, the Middle East, and West Africa. With the availability of inexpensive clay pipes, tobacco became an item of mass consumption in England as early as 1670. Pipe manufacture spread throughout Europe. By the end of the 18th century, Dutch towns such as Gouda could support 350 pipe manufacturers, thanks to the smoking culture of coffeehouses and alehouses. snuff also proliferated, often rivaling smoking as the dominant form of tobacco consumption and producing such fascinating novelties as the perhaps apocryphal but frequently cited special pockets in the clothes of Frederick the Great (Frederick II) of Prussia, which were enlarged to cope with his considerable consumption. In southern Europe the great state-owned tobacco factories of Cádiz and Sevilla ensured the continued popularity of the cigar, though it was not until the Peninsular War (1808–14) that military officers began to popularize it in Britain. When pipes (pipe) were introduced into Asia, they were quickly adapted and made from materials as diverse as wood, bamboo, jade, ivory, metal, and porcelain. Arab communities took up the hookah, or water pipe, and smoking became a shared activity typically enjoyed with conversation and coffee. The hookah spread throughout Persia (present-day Iran) and into India, eventually reaching China, Southeast Asia, and many parts of Africa by the end of the 17th century. By the mid-19th century, smoking had become an established ritual throughout the world. It was celebrated in prose, in verse, in art, and on the stage, and its use came to be seen as a central component of manhood. Literary sources captured the paraphernalia of the smoking ritual—pipes, cleaners, holders, spills, spittoons, ashtrays, pouches, storage jars, and lighters, as well as smoking jackets, armchairs, hats, and slippers—all of which, ideally, had to be collected in “that chamber of liberty, that sanctuary of the persecuted, that temple of refuge… the smoking room” ( Ouida, Under Two Flags, 1867).The age of the cigarette
Mass production and mass appeal
 Cigarettes were originally sold as an expensive handmade luxury item for the urban elites of Europe. However, cigarette manufacture was revolutionized by the introduction of a rolling machine called the Bonsack machine, which was patented by American James Bonsack in the United States in 1880. The machine was soon put into use by the American industrialist James Buchanan Duke (Duke, James Buchanan), who founded the American Tobacco Company (ATC) in 1890. Inexpensive mass-produced cigarettes, promoted by Duke's aggressive marketing methods and advertising, gradually led to a decline in pipe-smoking and tobacco-chewing habits in the United States. In Britain the manufacturer Henry Wills began using the machine in Bristol in 1883, and this enabled him to dominate the cigarette trade within just a few years. Then, in 1901, Duke attempted to enter the British market. The subsequent “tobacco war” resulted in a standoff as the British manufacturers united within the Imperial Tobacco Company. An agreement in 1902 allowed both sides to claim a victory. Duke retreated to the United States, and the British market was left to Imperial, but together they formed the British-American Tobacco Company (British American Tobacco PLC) (BAT) to market and sell their products to the rest of the world, especially India, China, and the British dominions. Although other American companies entered the global market following the breakup of the ATC—the result of a 1911 Supreme Court ruling under the Sherman Antitrust Act (1890)—BAT continued to meet much success. In 1999 the company produced more than 800 billion cigarettes per year, which made it the world's third largest tobacco company (just behind the Philip Morris USA and Philip Morris International companies, together ranking second, and the China National Tobacco Corporation, ranking first).
Cigarettes were originally sold as an expensive handmade luxury item for the urban elites of Europe. However, cigarette manufacture was revolutionized by the introduction of a rolling machine called the Bonsack machine, which was patented by American James Bonsack in the United States in 1880. The machine was soon put into use by the American industrialist James Buchanan Duke (Duke, James Buchanan), who founded the American Tobacco Company (ATC) in 1890. Inexpensive mass-produced cigarettes, promoted by Duke's aggressive marketing methods and advertising, gradually led to a decline in pipe-smoking and tobacco-chewing habits in the United States. In Britain the manufacturer Henry Wills began using the machine in Bristol in 1883, and this enabled him to dominate the cigarette trade within just a few years. Then, in 1901, Duke attempted to enter the British market. The subsequent “tobacco war” resulted in a standoff as the British manufacturers united within the Imperial Tobacco Company. An agreement in 1902 allowed both sides to claim a victory. Duke retreated to the United States, and the British market was left to Imperial, but together they formed the British-American Tobacco Company (British American Tobacco PLC) (BAT) to market and sell their products to the rest of the world, especially India, China, and the British dominions. Although other American companies entered the global market following the breakup of the ATC—the result of a 1911 Supreme Court ruling under the Sherman Antitrust Act (1890)—BAT continued to meet much success. In 1999 the company produced more than 800 billion cigarettes per year, which made it the world's third largest tobacco company (just behind the Philip Morris USA and Philip Morris International companies, together ranking second, and the China National Tobacco Corporation, ranking first).The success of the cigarette was due not only to the business strategies of the large firms but also to the rapid adoption by urban male youths of the relatively inexpensive and easy-to-smoke lighter flue-cured Virginia tobacco. In particular, this product became a favourite of teenage boys—a situation that led to public outcries, to the revival of antitobacco movements in France, Australia, Britain, Canada, and the United States (spearheaded there by the seasoned antidrink campaigners of the Woman's Christian Temperance Union), and to the eventual passing, in the 1890s and 1900s, of legislation across most territorial and federal states banning the sale of tobacco to minors. The legislation, however, was largely ineffective, and World War I quickly put an end to the critique of young men's cigarette smoking. In the trenches cigarettes were easier to smoke than pipes, and tobacco companies, the military, governments, and newspapers organized a constant supply of cigarettes to the troops—an official recognition of the importance of tobacco in offering immediate relief from physical and psychological stress. Certain companies did extraordinarily well from the war: Imperial's Players and Woodbine brands in Britain and, more spectacularly, R.J. Reynolds (R.J. Reynolds Tobacco Holdings)'s Camel in the United States. Introduced only in 1913, Camel had reached sales of 20 billion cigarettes by 1920, following a government supply order and a successful marketing campaign. The war, therefore, transformed smoking habits. As early as 1920, more than 50 percent of the tobacco consumed in Britain was in the form of cigarettes. A less-urban U.S. population lagged behind, but a similar story in World War II saw cigarettes achieve more than 50 percent of all tobacco sales in 1941. Several other industrial countries matched this trend.
 The first half of the 20th century was the golden age of the cigarette. In 1950 around half of the population of industrialized countries smoked, though that figure hides the fact that in countries such as the United Kingdom up to 80 percent of adult men were regular smokers. Smoking was an acceptable form of social behaviour in all areas of life—at work, in the home, in bars, and at the cinema—and advertisers were keen to show the full range of leisure activities made complete only through the addition of a cigarette. Smoking cigarettes was popular across all social classes and increasingly among women, once associations of smoking with deviant sexuality began to fade in the 1920s. This development had less to do with the efforts of advertisers—who, for example, in 1925 introduced the Marlboro brand as a woman's cigarette: “Mild as May”—and more to do with the impact of war and a direct confrontation with societal attitudes by so-called new women. Most important, the cigarette habit was legitimated, celebrated, and glamourized on the Hollywood screen and transported to the rest of the world. Movie (motion picture, history of the) stars such as Edward G. Robinson, James Cagney, Spencer Tracy, Gary Cooper, and especially Humphrey Bogart (Bogart, Humphrey), Lauren Bacall, and Marlene Dietrich raised the image of the cigarette to that of the iconic, ensuring it would never lose its sophisticated and loftily independent connotations.
The first half of the 20th century was the golden age of the cigarette. In 1950 around half of the population of industrialized countries smoked, though that figure hides the fact that in countries such as the United Kingdom up to 80 percent of adult men were regular smokers. Smoking was an acceptable form of social behaviour in all areas of life—at work, in the home, in bars, and at the cinema—and advertisers were keen to show the full range of leisure activities made complete only through the addition of a cigarette. Smoking cigarettes was popular across all social classes and increasingly among women, once associations of smoking with deviant sexuality began to fade in the 1920s. This development had less to do with the efforts of advertisers—who, for example, in 1925 introduced the Marlboro brand as a woman's cigarette: “Mild as May”—and more to do with the impact of war and a direct confrontation with societal attitudes by so-called new women. Most important, the cigarette habit was legitimated, celebrated, and glamourized on the Hollywood screen and transported to the rest of the world. Movie (motion picture, history of the) stars such as Edward G. Robinson, James Cagney, Spencer Tracy, Gary Cooper, and especially Humphrey Bogart (Bogart, Humphrey), Lauren Bacall, and Marlene Dietrich raised the image of the cigarette to that of the iconic, ensuring it would never lose its sophisticated and loftily independent connotations.The antismoking movement
Within this culture there was little room for opposition to tobacco, except in the privately financed publications of such antismoking cranks as the American industrialist Henry Ford and in the hysterical whims of the German leader Adolf Hitler—although the latter's state-sanctioned attack on the people's habit did lead to some pioneering work on the links between smoking and cancer. In 1950, works by the German-born American physician Ernst L. Wynder and by the British statisticians Austin Bradford Hill and Sir Richard Doll provided firm evidence linking lung cancer with smoking. This information came as a considerable shock to smokers, who proved reluctant to give up their habit. Of course, their decisions had already been influenced by physical addiction, advertising, and the denials of the tobacco industry, but, even after the reports by the Royal College of Physicians (1962) and the U.S. surgeon general (1964) clearly stating the deleterious health effects of smoking, quitting rates were not as high as might have been expected. An average of two million persons gave up smoking every year in the United States in the decade after 1964, but about half that number also began smoking every year, and not all quitters were able to remain nonsmokers. By 1978 the percentage of adults in the United States who smoked had fallen to 33 percent. A significant majority of those who had quit smoking were professional, affluent men, which made smoking a health problem increasingly associated with women and poverty. Whereas the average American smoker went through 22 cigarettes a day in 1954, the number had increased to 30 a day by 1978—a statistic that suggested that the quitting rate was higher among those who smoked less and that the increasing number of smokers who had moved to lighter or filtered brands were smoking more of them.
More recent evidence of the harm done to nonsmokers by environmental tobacco smoke has further helped turn attitudes against smoking. Efforts to curtail the individual's liberty to smoke were at first most pronounced in the United States, as in California's 1995 ban on smoking in most enclosed places of employment, but in 2004 Ireland became the first country to ban smoking in enclosed workplaces, and other countries have since followed suit. Nevertheless, the strong grip of smoking on the world's popular culture suggests that the practice will persist. While smoking is increasingly frowned upon in a health-conscious age and the smoker has come to feel marginalized and harassed, the very suppression of smoking only increases its power as a symbol of individualism and resistance. For instance, a survey of internationally successful Hollywood films (motion picture, history of the) found that motion pictures released in 1995 featured four times as much smoking as those released in 1990, with an increase in the number of positive verbal and visual references made to the habit. These images are being broadcast to the very areas of the world where American-owned tobacco companies are beginning to make inroads selling their products. All this suggests that smoking is likely to remain as entrenched in modern global society as it was in pre-Columbian America. Cigarette use might now be more individualistic and less ceremonial than it was at that time, but this change too is a reflection of the transformation of culture to one that has come to value individualism over tradition. Mark Twain (Twain, Mark)'s famous quip regarding his own smoking habit (estimated to have reached more than 20 cigars per day) might be applied to the complex status of smoking in society today:To cease smoking is the easiest thing I ever did. I ought to know because I've done it a thousand times.Additional Reading
Smoking and health
American Lung Association, 7 Steps to a Smoke-Free Life (1998), provides a practical approach to helping a smoker quit that anticipates the difficulties and potential setbacks many smokers will face in achieving this goal. Ronald R. Watson and Mark Witten (eds.), Environmental Tobacco Smoke (2001), discusses in scientific detail the effects of tobacco smoke on nonsmokers and also the broader issues concerning the reduction of exposure to environmental tobacco smoke.
Smoking and public policy
Kathleen R. Stratton et al. (eds.), Clearing the Smoke: Assessing the Science Base for Tobacco Harm Reduction (2001), explores various smoking-related products claimed to reduce the health risks associated with tobacco smoke, focusing on the products' effectiveness and suggesting ways that policy makers and other officials should evaluate them. World Bank, Curbing the Epidemic: Governments and the Economics of Tobacco Control (1999), looks at the economic measures available to policy makers to control smoking and assesses the economic consequences associated with a reduction of tobacco consumption. Robert L. Rabin and Stephen D. Sugarman (eds.), Regulating Tobacco (2001), presents a collection of essays dealing with the large array of public policy issues on smoking, including cultural and political questions concerning its regulation.
History of smoking
Jordan Goodman, Tobacco in History: Cultures of Dependence (1993), provides the most wide-ranging global history of tobacco from Native American society to the present. Richard Kluger, Ashes to Ashes (1996), provides a comprehensive history of smoking in the 20th-century United States. Matthew Hilton, Smoking in British Popular Culture, 1800–2000 (2000), focuses on smoking in Britain, although its thorough account of the social history of smoking over the past two centuries also applies to other national contexts.
- Sant Fateh Singh
- Santhāl
- Santiago
- Santiago, Battle of
- Santiago Calatrava
- Santiago Carrillo
- Santiago de Compostela
- Santiago de Cuba
- Santiago del Estero
- Santiago de los Caballeros
- Santiago de Surco
- Santiago, Order of
- Santiago Ramón y Cajal
- Santiago Rodríguez
- Santiago, Río Grande de
- Santillana, Iñigo López de Mendoza, marqués de
- Santipur
- Santo André
- Santo Antão Island
- Santo Domingo
- Santonian Stage
- Santorio Santorio
- Santos
- Santos-Dumont, Alberto
- Santos-Dumont No. 14-bis